

Testosterone Isn't Just About Sex. It's About Not Dying.
Inside the FDA's first-ever men's health panel - and the facts we've all been ignoring for decades.


“We have a men’s health crisis in this country.”
Well, that’s something I thought I’d never hear a senior government official say out loud.
2 days ago the Assistant Secretary for Health, Admiral Brian Christine, stood in front of an FDA panel and said it unapologetically.
Then he showed us the numbers.
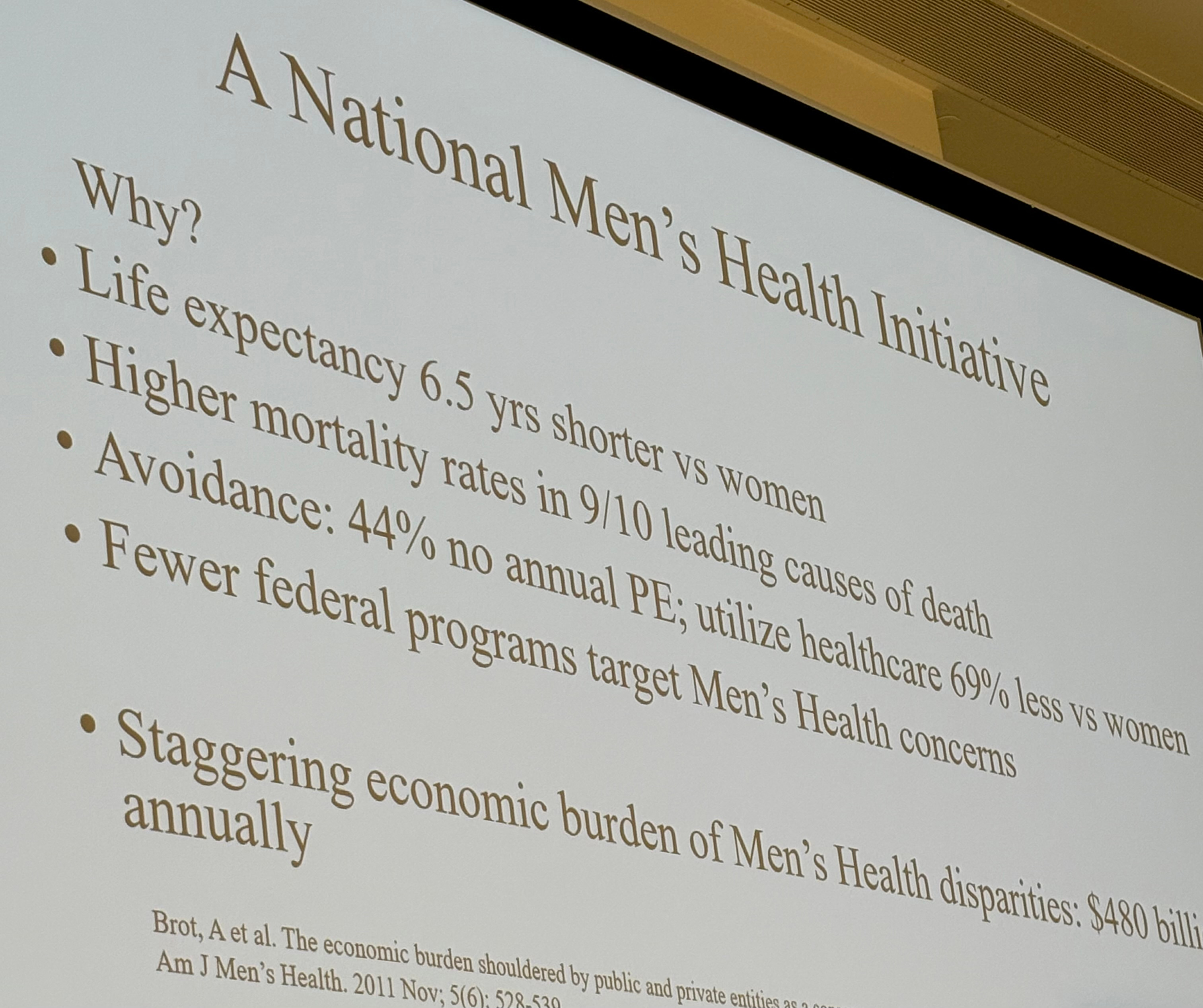
Men die 6.5 years earlier than women. They have higher mortality rates in 9 of the 10 leading causes of death. 44% don’t get an annual physical. They use healthcare resources 69% less than women.
And 100 men per day take their own lives. Almost 80% of all suicides are male.
Six million men experience depression annually- roughly the same as women- but only 25% seek treatment.
The economic burden of ignoring all this? Almost $500 billion a year.
I sat surrounded by some of the top urologists, endocrinologists, and researchers in the country and thought, this should be front-page news.
But instead, of course, almost no one covered it.
Let me tell you what was said.
We talked a lot about testosterone.
When most people hear “testosterone therapy,” they think sex. Erectile dysfunction. Some guy trying to relive his twenties.
But that framing costs men their lives.
Testosterone deficiency isn’t just some sex problem. It’s a metabolic problem. A cardiovascular problem. A bone problem. A mortality problem.
Just take a look at the numbers presented by Dr. Mohit Khera.
Men with low testosterone are.
17% more likely to have cardiovascular disease
50% more likely to have diabetes
50% more likely to break a bone
69% more likely to have obesity
86% more likely to suffer from depression
In the ER, I treated the downstream consequences every shift. The diabetic whose foot ulcer won’t heal. The 68-year-old who broke a hip and will never walk independently again. The guy having his second heart attack at 55
But what I didn’t realize until much later is that many of those cases trace back to a condition we aren’t even screening for - and actively shame men for even asking about.
Entirely treatable testosterone deficiency.
But doesn’t testosterone replacement do more harm than good?
The panel addressed this question over and over.

They walked through studies that should have changed medicine years ago.
The biggest one (TRAVERSE) looked at 5,246 men. Gold-standard research. Published in the New England Journal of Medicine in 2023.
What they found was that proper testosterone replacement therapy (TRT) didn’t actually cause a lot of the horrible things that we’ve always told men it does. Didn’t cause heart attacks. Didn’t cause prostate cancer. Didn’t make urinary problems worse.
The VA also looked into TRT. They tracked over 80,000 men with low testosterone and found that TRT that normalized testosterone was associated with 56% lower ‘all-cause mortality.’
In plain English:
Effectively treating testosterone deficiency was associated with being less likely to die… from anything. These men also suffered fewer heart attacks. Fewer strokes.
Here’s some data that haunts me personally given how often I’ve admitted these men from the ER:
1 in 4 men over 50 develop osteoporosis.
Two-thirds of elderly men who break a hip have low T.
And when an elderly man breaks his hip, there’s a 1 in 3 chance he’s dead within a year.
One in three. And we’re still not paying attention.
The Fairy Tale That Started It All
Dr. Abraham Morgentaler from Harvard didn’t mince words.
He called the demonization of testosterone “a tragedy,” the dismissal of men suffering from it “a scandal,” and the failure to teach it to medical students “a stain on my generation of medical educators.”
Then he explained where the fear came from.
In 1941, Charles Huggins- who would later win a Nobel Prize for his research- claimed testosterone acted as a “prostate cancer accelerator.”
His evidence? Well. One patient. Treated for less than three weeks.
For 60 years, the entire medical establishment operated on that assumption.
And over the last 30 years, the evidence has repeatedly, uniformly, and overwhelmingly shown it to be false. Not a single large trial shows increased prostate cancer risk. Several show decreased risk.
But the narrative still lives on as false narratives often do.
“FOLLOW THE SCIENCE,” they scream.
Well, we’re finally trying, and Morgentaler’s conclusion left no room for doubt.
“In 2025, the belief that testosterone is dangerous for the prostate is no more scientifically valid than belief in the tooth fairy.”
The FDA finally removed the cardiovascular warning in February 2025.
But the prostate warnings remain on the label- based on one man studied for less than three weeks in 1941 and despite buckets of evidence since that states the opposite.
We should look into that.
And now for the ‘controlled substance’ absurdity
Testosterone- the hormone your body makes naturally- is classified as a Schedule 3 controlled substance. Right alongside ketamine. More tightly regulated than benzodiazepines. With zero evidence of dependency at replacement doses.
The Anabolic Steroid Control Act of 1990 that initiated the testosterone lockdown was a political response to Olympic doping scandals and bodybuilding culture.
The images that drove this policy? Terminator, Rambo, Ben Johnson losing his medal.
Culture was the “scientific basis” for treating testosterone like a narcotic.
Weird.
And like many examples of government regulation: it didn’t even work.
Within 10 years, illicit steroid use exceeded pre-legislation levels, but no one ever thought to revisit.
What it did do was create a gauntlet for the 60-year-old man seeking legitimate treatment.
One panelist described it well.
Patient shows up already embarrassed. The doctor looks you up in the controlled substances registry. The pharmacy won’t carry it. Another pharmacy will only fill one month. Everyone treats you like a drug seeker.
The whole process takes someone seeking medical care and makes them feel like an addict.
And for what purpose? Who are we saving here?
Meanwhile, estrogen, progesterone, thyroid hormone, cortisol, growth hormone- all free from bullshit restrictions. Testosterone is the only natural hormone treated like a street drug.
What This Information Means For You
If you’re a man- or if you love one- here’s what that room full of experts agreed on:
Get tested. Testosterone should be part of routine bloodwork, like cholesterol and blood sugar. If you’re over 40, get a baseline. If you have diabetes, obesity, metabolic syndrome, or depression, get tested now.
The benefits are real. For men who are deficient, testosterone therapy can improve bone density, blood sugar control, mood- and according to the VA data maybe even the likelihood of living a longer life.
Many risks were overblown. The prostate cancer fear was based on one patient in 1941. The cardiovascular warnings were removed earlier this year after major trials showed no increased risk.
This risk is serious and real. Testosterone can shut down sperm production quickly, even at low doses. If you’re younger and might want kids, you need to discuss this before starting treatment. There are ways to manage it, but you have to plan ahead.
What needs to change. Remove the outdated prostate warnings. Take testosterone off Schedule 3. Eliminate the FDA requirement for a clinician to know why a man has low T before treating him (the one that excludes 89% of men with low testosterone from approved treatment.)
Final thoughts.
There are many ways to raise testosterone ranging from lifting heavy and reducing stress to prescription treatments, but knowing more about it and what your baseline is helps YOU make better decisions with your doctor (and maybe your trainer) to get where you need to be. And by all means, avoid the online supplements and pop-up T clinics. Those are NOT your best options.
Admiral Christine told us he was flying back to Washington after Thanksgiving a few weeks ago, sitting in plain clothes next to two women he didn’t know.
During the flight, one started talking to the other about the recent FDA changes to hormone therapy labeling for women. Two strangers, caught in the wild just chatting about how the government was finally telling them the truth.
Imagine that.
Four weeks ago, the FDA admitted they’d been wrong about hormone replacement therapy in women for 23 years. And they fixed it. I was proud.

Having been in the room when those decisions were announced (sitting across from the Second Lady!! *swoon*), I wrote about the experience in an article you can find here.
Now this week, the FDA acknowledged the parallel disaster for men, and that’s a good thing. Because that’s how we move forward.
But the remaining question is whether FDA and HHS will launch a National Men’s Health Initiative and actually do what is necessary to serve our nation’s men - or whether we’ll be stuck waiting another 23 years.
My take? It must be now. Men are running out of time.
If you enjoyed this article, please consider sharing it with a friend (or your doctor). And here’s the link to the YT video of the FDA Panel’s full discussion. Check it out.
Just found out that Substack allows for a pinned comment!
Would appreciate hearing your perspective on this counter argument.
https://open.substack.com/pub/gooznews/p/makarys-fda-stacks-another-panel?r=44uij&utm_medium=ios